


Med Students
The landscape of American health care is shifting beneath our feet. And if anyone pretends to know where it is going, they’re fooling themselves. Private insurers thought they would make out well, but the low enrollment on health exchanges puts them at risk. Democrats thought once the legislation rolled out and the benefits were seen more clearly that it would be another irremovable plank for the social safety net. Republicans secretly thought they could keep campaigning against Obamacare without ever having to actually fix it. Everyone was wrong.
Who would have thought a website could put a presidency and 17% of our national economy in such a state of uncertainty?
But this essay is not my analysis of Obamacare. Nor is it my prediction of what is ahead for private health insurance or the single-payer pipedream or a political analysis of who benefits and how from the debacle. It’s a question for young physicians, medical students, and the med school hopefuls out there.
The question I have is: Why do you want to be a physician?
* * *
Medical school applicants will recognize this question. It’s the central one we all pondered as we plugged coursework into the application system and studied for the MCAT. As a faculty member at Saint Louis University I was on the pre-med evaluation committee and advised many pre-med students. So I have read my fair share of these essays; and they largely revolve around one idea: applicants say they want to put their gifts at the service of others. Some had a life-changing moment, others just love science, and many had family members who inspired a love of medicine. But almost everyone talks about service.
On top of all the health care-related stories, we’re about to hear another one that’s again going to make you question the promises of reform. It’s possible that 10 million people will gain coverage through Medicaid over the next year. Medicaid is an essential program for the poor and disabled, but is notorious among the medical community for its low and slow reimbursement of their services. Therefore, many physicians won’t accept new Medicaid patients. For example, in New Jersey, only 40% of physicians will accept them. Let me say that again – only 40% of the doctors in New Jersey will see new patients covered by insurance for the poor and disabled.
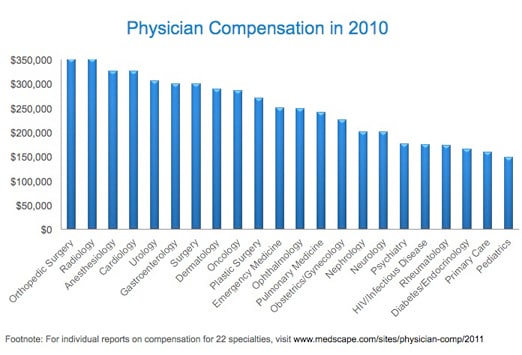
This isn’t the only issue related to access to health care: the workforce for preventive medicine and primary care has yet to be adequately expanded; we have yet to crack the code of how to maintain quality care in rural areas; the disparity in compensation between specialties is well-established, and as a result, it will often be even more difficult for Medicaid patients to access. And so on.
* * *

Rising medical costs
So what’s the solution to this impending problem? How are we to ensure that even after this first step of reform the poor and disabled don’t get left standing on the outside looking in? There are policy levers that physicians would like pulled: reforming malpractice, reducing paperwork, instituting a co-pay. But what we could really use is genuine moral leadership from our physicians.
While teaching at Saint Louis University, I distinctly remember one afternoon when I was discussing health care reform with a public health class that largely consisted of pre-med students. I was explaining some of the policy changes in the Affordable Care Act and they were slowly realizing how much the medical profession could change before they ever completed medical school. But they were also realizing how complex the whole system was. At one point I stepped back and said, “The truth is, once you get an M.D. behind your name, you are going to have a much louder voice on health policy than anyone else. Once you graduate from medical school, people will look to you for leadership on these issues even if you don’t know what you’re talking about. So, please, know what you are talking about and use your voice to speak for those who can’t.” The class was filled with compassionate, bright students and we will count on their leadership very soon.
The sad truth is that we have a very dispiriting history of physicians and health care reform. Anyone interested in the full story has to read The Social Transformation of American Medicine by Paul Starr. This Pulitzer and Bancroft award-winning book is a tour de force that deserves to be read by every medical student. One takeaway of Starr’s history is that the physician community has a great track record of looking out for itself rather than the patients it serves. It has regularly used its power of advocacy to ensure its social status and financial compensation were protected above all else. (And yes, I realize a member of the clergy making that critique is like the pot calling the kettle black.) It will be interesting to see how the physician community understands this impending crisis of care.
In particular, I am interested in who is at the center of questions and solutions. The patient? Or the provider?
A patient-centered question is – how do we make sure everyone on Medicaid has access to the care they need?
A provider-centered question is – how do we make sure those who see Medicaid patients are fairly compensated for their time?
They’re not mutually exclusive ideas, but they’re very different starting points. The problem is we screen med school applicants with a provider-centered question – “Why do I want to be a physician?” That’s only half the equation. I think the truth in all of this is that most who practice medicine would be willing to see Medicaid patients, but they feel trapped in a system that makes doing so very difficult. As we look to fix that, can we place patients rather than physicians at the center of the system? You’ll notice I haven’t proposed any specific policy changes myself. All I’ve done is asked whose interest ought to be foremost on our mind.
* * *
I can anticipate the main concern of the medical students and young physicians. They are saddled with massive debt and the situation is only getting worse. It’s hard to choose a poorly paid (but desperately needed) specialty or live in poorly compensated (but in need of a doctor) area or see poorly reimbursed (but very ill) patients when you are worried about over $150,000 of educational debt. If I had a health policy wand, it is one of the first things I would change. Moreover, many physician-owned practices already operate on a razor-thin margin. So, many might believe in the moral imperative to care for those who most need it, but they can’t afford to do so.
I said in the beginning that anyone who predicts where this thing is going is delusional. So I am not predicting. I’m speculating. And, if the historical pattern of successful, self-interested advocacy by physicians holds, I’ll be absolutely wrong.
I think, after massive hysteria from physicians, it will be far less likely that a physician is extremely wealthy. Generalists will be paid about the same as today, but specialists will be paid less. There will be panic that medicine will no longer attract the most capable people, but that’ll just be a smokescreen for those who are afraid their own compensation will decrease. There will be cries that scientific advances will lessen because specialties and technology will not be incentivized (and that one might actually be true).

“Who needs me to be a physician?”
Yet the salary squeeze, I suspect, will make it less likely that financial or social status motives will drive students into the field. The test scores of applicants might be slightly lower, but they’ll make better doctors in the end. Patients across the socio-economic spectrum will have more confidence in their providers and physicians might start rivaling nurses in public trust. And those aspirants to medical school who write, “I want to be a physician because I want to put my gifts at the services of others,” will actually get to give their gifts to the other who needs it most.
Many of my close friends have sacrificed a great deal to complete rigorous training and continue to make tremendous sacrifices to care for people in their most desperate hour. But for those who feel stuck in a system that they think prevents them from seeing the poor, I believe that physicians might be the only ones capable of changing it.
So, to those just starting out in medicine. Even though you won’t see it on your med-school applications, there is a question just as important as, ‘Why do I want to be a physician?’ It is, ‘Who needs me to be a physician?’ Once again, different starting points, but the two should go together. The future is uncertain, but for those who can answer these questions honestly, there is no need for panic. Just read this article again and call me in the morning.
* * *
Editor’s note: the cover image for this piece is available from a.drian at Flickr available here

{kind=link}
{kind=link}